The Pittsburgh Center for Plastic Surgery is primarily an aesthetic surgical practice, focusing on providing outstanding cosmetic results to our patients. We understand that at times, certain procedures may fall under the umbrella of medical necessity, and we are happy to provide that service to our patients. Below is information to understand our office’s criteria for coverage.
Common Criteria
Medical Necessity: For any surgical medical procedure to be covered by insurance, it must be deemed medically necessary by a qualified healthcare provider(s), which is generally your surgeon. At times, more than one provider may be required to determine medical necessity, including primary care or other physicians. Medical necessity is not determined by an insurance company or plan.
Pre-Authorization: An insurance company then authorizes a procedure based on the declaration of medical necessity. This usually involves submitting a letter of medical necessity from the healthcare provider, along with the patient's medical records and other required documentation. We will not submit for pre-authorization without all required documentation.
The insurance company then matches this documentation against their pre-set criteria for coverage which is specific to your insurance plan, and they determine if your plan is eligible for coverage of that medical necessity. If you have questions about your insurance plan’s criteria you must contact the insurance plan directly.
Documentation of Symptoms: Detailed medical records are usually necessary, including photos, showing that the patient has experienced symptoms due to the medical condition which requires surgery. The duration and severity of symptoms required to authorize a procedure can vary between insurance, even if your symptoms may meet medical necessity.
Non-Surgical Treatment Failure: Many insurance companies require proof that non-surgical treatments have been tried and failed for a specified period of time.
Age: Some insurance companies have age restrictions, either requiring patients to be over 18 or, in some cases, over 21.
BMI: Many insurance companies have BMI cutoffs to reduce risks for complications associated with medically necessary procedures, as higher risk patients may require more extensive surgical management then is usually covered. At our office, to be considered medically necessary your BMI must be less than 35.
Nicotine Use: As patients who utilize nicotine containing products have a higher than normal rate of complications associated with surgery, no procedure will be considered medically necessary if the patient utilizes nicotine. The patient must demonstrate cessation at least 6 weeks prior to surgery via nicotine level tests to have a surgery authorized. Any positive tests prior to surgery will lead to cancellation of surgery.
Individual Criteria
- A breast reduction involves removal of breast tissue from the breast to reduce it in size. It includes removal of an equivalent amount of skin, to reshape and lift the breast.
- Breast reductions do not include removal of Non-breast tissue (i.e. fat) from portions of the breast or outside of the breast, like the lateral chest. These additional areas are considered cosmetic, but are often necessary to obtain a good cosmetic result.
- For example, just reducing the breast (cup size), but not reducing the chest (strap size) can lead to an appearance of disproportion between the breast and chest, and is a common cause of patient dissatisfaction.
- The following are breast reduction criteria:
- The patient has had ongoing evaluation by a primary care physician who has ruled out causes unrelated to breast hypertrophy
- At least three months of conservative treatment which has failed to relieve symptoms.
- Symptoms include: Back, neck, or shoulder pain, bra grooving, rashes or skin problems between or under the breasts, impairment of regular activities, etc.
- Conservative treatment includes such therapeutic measures as: analgesics/anti-inflammatory medications, physical therapy, appropriate support bra, therapeutic exercises, weight loss, heat or cold application, etc.
- Letter(s) of medical necessity from other healthcare professionals (primary care physician, physical therapist, chiropractic physician and orthopedic surgery) stating that your symptoms remain refractory after other treatments have been tried and failed to relieve symptoms.
- For women over 40, a copy of your most recent mammogram report.
- Patients must have an expected reduction of approximately 350 grams (approximately 1-2 cup sizes) minimum to meet medical necessity. Patients may be required to have a higher gram requirement that is based on body surface area known as the Schnur scale, roughly described below:
| BSA | Grams |
| 1.6 | 350 |
| 1.75 | 400 |
| 1.85 | 500 |
| 1.95 | 600 |
| 2.05 | 700 |
| 2.15 | 850 |
| 2.25 | 1000 |
| 2.35 | 1200 |
| 2.45 | 1400 |
- A panniculectomy is removal of the hanging skin (abdominal pannus) below a fold of the abdomen that is interfering with daily function of a patient. As the skin is hanging, its removal does not tighten the skin of the abdomen, or the abdominal muscles. It is NOT a cosmetic procedure and frequently confused with a tummy tuck (abdominoplasty).
- An abdominoplasty removes skin up to the belly button and sometimes above the belly button. It is a procedure to tighten the skin of the abdomen and the abdominal muscles. Since removal of the skin is up to the belly button, this often includes the skin of the abdominal pannus even if panniculectomy is not individually listed on the surgical plan.
- To avoid unnecessary charges and avoid complexity of the insurance pre-authorization to the patient, a panniculectomy is only charged to the patient or insurance if the abdominal pannus is large enough that it requires additional surgical time, surgical labor, or modification of standard abdominoplasty technique.
- Common Misconceptions:
- Myth: Insurance pays for “part of” a tummy tuck (abdominoplasty) surgery.
- Fact: Insurance covers a procedure based on code (CPT). They cover the entire code of the surgery, minus co-pays, deductibles, or co-insurance. The panniculectomy code is 15830 and the abdominoplasty code is 15847. The amount the insurance pays cannot be applied to another surgery code that is considered cosmetic.
- Myth: My doctor told me my tummy tuck is fully covered under insurance.
- Fact: Some surgeons bill insurance for a panniculectomy, but then perform some of an abdominoplasty. This is often an incomplete abdominoplasty procedure that takes short cuts and can result in an incomplete result. It is difficult to revise these procedures into full tummy tucks if they do not give a good cosmetic outcome because of these short cuts. It is also insurance fraud and can result in criminal penalties.
- Myth: I am saving money by using insurance for the panniculectomy.
- Fact: Some surgeons “double charge” patients for an abdominoplasty and a panniculectomy and then give them discounts so patients believe they are “saving” money, but in fact are getting charged extra for something that is often included. Patients receive a surprise bill for the panniculectomy after surgery that can be very expensive in high deductible plans. Our office will only charge for the panniculectomy if it adds additional labor, and we will provide clear and detailed estimates of your costs and coverage.
- If you require a panniculectomy, the following criteria must be met:
- The medical records by a primary care physician document that the panniculus or fold causes chronic intertrigo (dermatitis occurring on opposed surfaces of the skin, skin irritation, infection or chafing) and often requires a positive culture (bacterial or fungal) and that consistently recurs or remains refractory to appropriate medical therapy (including appropriate prescription medications) over a period of three (3) months.
- Preoperative photographs document that the panniculus or fold hangs at or below the level of the symphysis pubis.
- Documentation of weight loss consisting of minimum 35% of excess body weight lost. Patients who underweight bariatric surgery must be 18 months post-operative, and have 6 months stability at the documented weight. All patients must have documented 6 months weight stability regardless of form of weight loss.
- The Women's Health and Cancer Rights Act (WHCRA) of 1998 requires insurance companies that offer mastectomy coverage also provide coverage for reconstructive surgery after mastectomy. This applies to patients who are undergoing mastectomy due to breast cancer. The Act covers:
- Reconstruction of the breast on which the mastectomy has been performed.
- Surgery and reconstruction of the other breast to produce a symmetrical appearance to the reconstructed breast in clothing
- Prostheses (breast implants or other devices to replace the removed breast).
- Physical complications of all stages of mastectomy
- Additional procedures which may be considered cosmetic in nature are not covered.
- The WHCRA does not specify reconstruction after lumpectomy, or other breast conserving therapies. Check with your insurance company regarding coverage.
- Rhinoplasty is generally considered to be a cosmetic procedure, which means it's typically not covered by insurance. However, a rhinoplasty may be covered under the following circumstances:
- Trauma: If the nasal deformity is the result of an accident or injury, insurance may cover the cost of rhinoplasty. This usually requires medical documentation from at the time of injury.
- Congenital Defects: If a person is born with a nasal defect that impairs their ability to breathe properly, insurance may cover the cost of surgery to correct the defect.
- Obstructed Breathing: If a person has difficulty breathing due to:
- Deviated septum, turbinate hypertrophy, or nasal valve collapse
- Insurance will generally cover specific procedures to address the breathing obstruction and will not cover the cost of the cosmetic portion of the rhinoplasty
- Symptoms must have been present for 12 months and not be responsive to conservative therapy.
- Upper Blepharoplasty involved removal of excess skin that may cause lid heaviness and difficulty with vision. Sometimes, the upper lids may obstruct vision because of muscle weakness (lid ptosis), and not because of excess skin. This requires treatment by an oculoplastic specialist in severe or asymmetric cases.
- On examination your surgeon may discover that your eyebrows hang low (brow ptosis). This often needs to be corrected at the same time as your blepharoplasty or in lieu of your blepharoplasty to avoid visual issues such as chronic dry eyes after surgery. Brow corrections (brow lifts) are most often not covered by insurance.
- If you require an upper blepharoplasty, the following criteria must be met:
- Clinical Documentation: Detailed clinical records documenting symptoms.
- This might include regular complaints of difficulty with activities such as reading, driving, or other daily tasks due to upper eyelid drooping.
- Visual Field Testing: Insurance companies usually require objective evidence of significant visual field obstruction. This typically involves formal visual field testing, which measures your central and peripheral (side) vision. Often, visual field tests need to be performed both with the eyelids in their natural position and then taped, to demonstrate significant improvement when the eyelids are lifted.
- Ophthalmologist or Optometrist Evaluation: An evaluation by an eye care professional is generally necessary to confirm the extent of visual field obstruction and the necessity of surgery.
- Photographic Evidence: Photographs of the eyes in their natural open position to visually document the eyelid droopiness (ptosis) or dermatochalasis (excess upper eyelid skin) that is impacting the visual field.
- Failed Non-Surgical Interventions: In some cases, insurance companies may require evidence that non-surgical treatments have been tried and failed. This might include the use of special glasses or tape to lift the eyelids.
- If your implants rupture before the end of life expectancy (<10 years since placement), most implant companies offer cash value coverage of replacement surgery based on the included or upgraded warranty you obtained at the time of implant placement.
- Removal of cosmetically placed breast implants after end-of-life expectancy of the implant is generally considered to be a cosmetic procedure, which means it's typically not covered by insurance. However, the procedure may be covered under the following circumstances:
- Trauma: If the implants have ruptured due to trauma. This usually requires medical documentation from including MRI or ultrasound imaging at the time of injury.
- Capsular Contracture: If implant rupture results in symptomatic Grade IV capsular contracture.
- Imaging: Insurance coverage required independent imaging, read by a radiologist confirming the rupture. The office will not supply this imaging and cannot formally diagnose rupture.
- Insurance may only cover removal for the ruptured side and not both implants. The office will also not replace cosmetically placed ruptured implants under insurance coverage, even if the ruptured implant removal is covered by insurance for the above circumstances.
- Many insurance plans do not cover gynecomastia surgical treatment. Please check with your individual plan regarding coverage. The diagnosis of gynecomastia must generally be made by a primary care or other supporting provider such as an endocrinologist. It should be supported by physical examination or ultrasound imaging/mammography.
- Patients must have documented symptoms including but not limited to breast pain/tenderness, discomfort in clothing, areolar enlargement, or nipple discharge. These symptoms should be present for a minimum of 6 months and are not responsive to conservative therapy.
- Laboratory examination of reversible causes of gynecomastia should be performed. Patients should have discontinued use of gynecomastia causing medications unless no alternative is available including but not limited to:
- Antipsychotics - Chlorpromazine, Fluphenazine, Haloperidol, Perphenazine, Thioridazine
- Calcium Channel Blockers - Verapamil, Nifedipine, Diltiazem
- Hormonal Blockers - dutasteride, finasteride
- Spironolactone, Marijuana, Anabolic Steroids
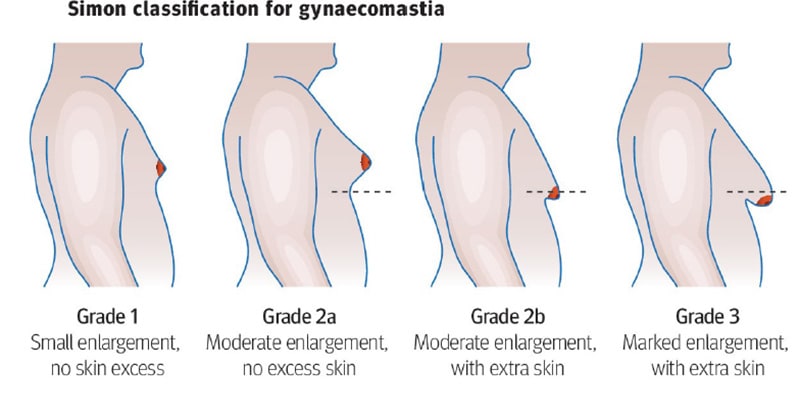
- Gynecomastia grade must be Simon Grade 2b or higher (Moderate enlargement with excess skin)
- Coverage is dependent on pathology results after surgery. Your claim may be denied if no breast tissue is present on the pathological exam. Pseudogynecomastia (adipose tissue only) is not covered.
- Many insurance plans do not cover gender affirming procedures. Please check with your individual plan regarding coverage.
- If your insurance plan covers these procedures, our office adheres to the standards outlined by the World Professional Association for Transgender Health (WPATH):
- Persistent Gender Dysphoria: Persistent, well-documented gender dysphoria is usually required.
- Medical and Mental Health Clearance: Many insurance companies require letters from healthcare professionals (often one from a mental health professional and one from a physician) attesting to the patient's readiness for surgery.
- Real-Life Experience: Some insurers require the individual to have lived continuously for 12 months in a gender role that is congruent with their gender identity (often referred to as the "real-life experience" or RLE).
- Hormone Therapy: If it's not contraindicated, 12 continuous months of hormone therapy as appropriate to the patient's gender goals (unless the patient has a medical contraindication or is otherwise unable or unwilling to take hormones).
- Our office offers “Top” surgery only. We do not offer facial masculinization or feminization surgery of any type.
- Gender Affirming top surgeries may involve other associated procedures to obtain the best cosmetic result. These procedures not covered by medical insurance, however if your surgeon’s plan requires these procedures to obtain the best result or reduce risk of surgery, surgery may not be offered if you decline the cash-pay component. Examples of these additional costs include:
- M2F
- Breast mesh placement to support large implants (>450 cc’s) or changes in position of the breast fold
- Fat grafting to augment native breast tissue naturally
- Liposuction to contour the lateral chest or axillary region
- F2M
- Excision or liposuction of non-breast tissue (i.e. fat) that extends into the lateral chest or axilla.
- Augmentation of the pectoralis muscles with fat
- Non excisional skin tightening procedures for areas of the chest that have loose skin but are not involved directly by the breast tissue.
- In our office, hernia repair is only performed in conjunction with other procedures which provide access to the hernia directly such as abdominoplasty, we do not perform isolated hernia repairs.
- Hernia repairs are charged to the patient or to insurance when the hernia is large enough that it requires additional surgical time, surgical labor, or modification of technique during a standard abdominoplasty.
- In order for the hernia repair to be covered under insurance, the patient must have a documented diagnosis of a hernia including imaging read by a radiologist such as an ultrasound, CT scan, or MRI demonstrating the hernia and discontinuity of the abdominal fascia.
Submission Process:
1) Prior to us submitting to your insurance for authorization you will need to meet the above requirements and have the documentation sent to our office. We will not send for authorization without the above documentation and requirements met. We recommend to have this documentation prior to your consultation so that there are no delays.
2) Once your insurance company has received our pre-certification package, it typically takes them up to one month to make a determination if your case meets their criteria for approval of benefits. Once your are authorized you will be contacted for a surgical date.
3) Our office does not determine your exact benefits package prior to surgery. We will provide a Good Faith Estimate (GFE), which outlines your expected charges with and without insurance coverage.
4) You are expected to pay any determined deductibles and/or any projected co-payment and co-insurances prior to scheduling your surgery.
5) If your insurance company receives our claim for your surgery, then later determines your surgery is cosmetic, and denies our claim for payment, you will be responsible for payment to the doctor, facility, and anesthesia.
6) If you wish to appeal a denial of surgery by your insurance company, we will provide you with our letter summarizing your medical necessity, but the appeal must be initiated and followed up by you.
7) We reserve the sole right to determine medical necessity based on our criteria and have the right to refuse surgery regardless of insurance pre-authorization if appropriate candidacy are not met, surgical risks are excessive, or of the scope of the requested or necessary surgery exceed typical insurance based surgical management.
Let Us Guide You
Our state-of-the-art facility is equipped with the latest technology and amenities to ensure your comfort and privacy during your visit. We are located in the heart of Pittsburgh and serve patients from all over the world. When you are ready to take the next step, contact us to schedule your consultation with Dr. Davila or Dr. Hurwitz. We look forward to helping you achieve your goals of looking and feeling your best.
Pittsburgh (Main) Office
3109 Forbes Ave, Ste 500,
Pittsburgh PA 15213
Mon - Fri: 8am - 4:30pm Saturday: By Appointment